


What’s the history of allergy shots and allergy drops?
Allergy immunotherapy (AIT) has been clinically practiced for over 100 years. The treatment was first tested on humans in 1911 when Leonard Noon injected patients suffering from hay fever with grass pollen-derived allergen extracts in increasing doses. This method was taken up rapidly all over the world by physicians trying to treat allergic diseases.¹
It wasn’t until the 1950s though that the first real clinical trials with allergen-specific immunotherapy were performed. In the next 30 years, allergen-specific immunotherapy grew in popularity around the world with different extracts and modalities being used.
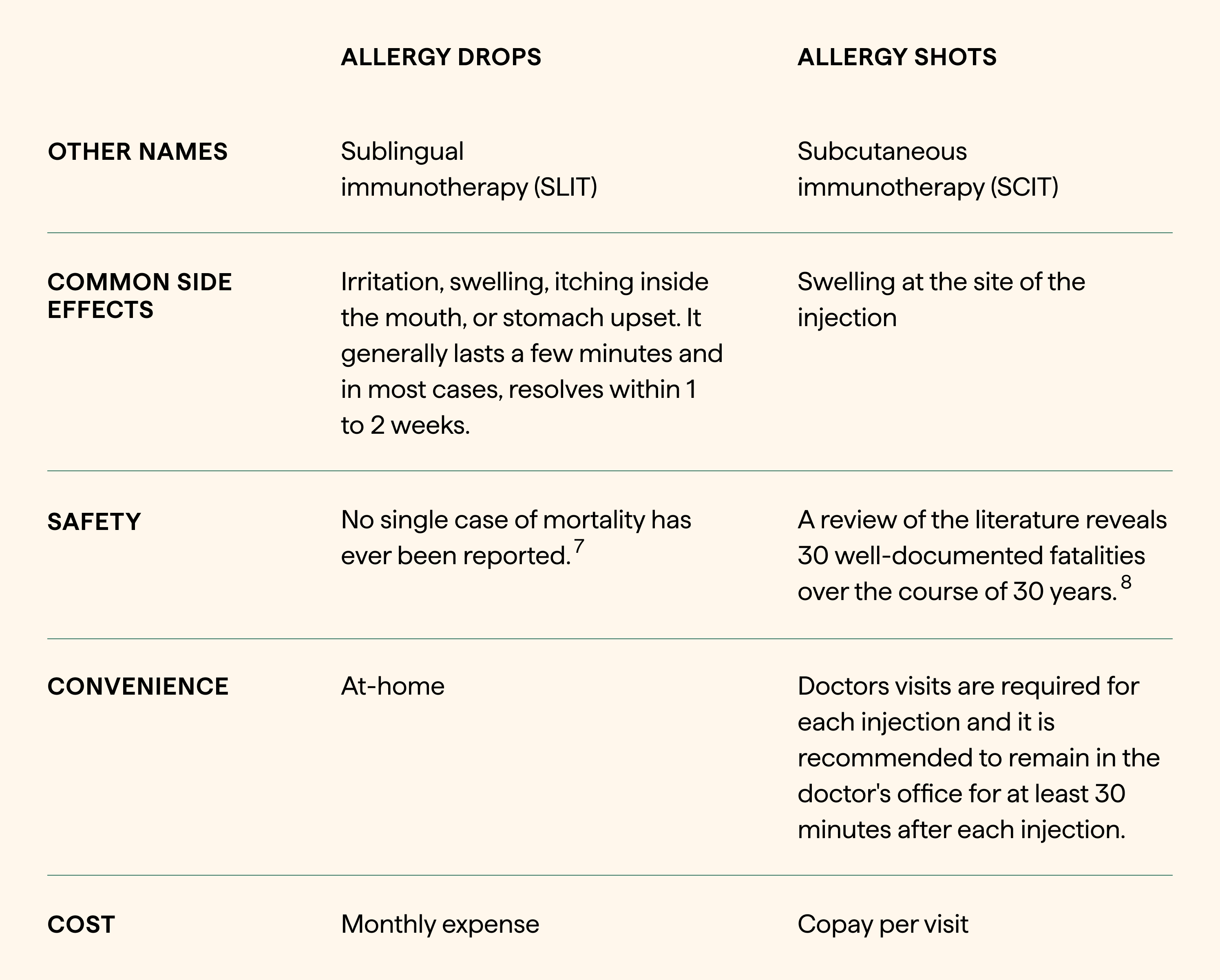
The two most common types of immunotherapy are subcutaneous immunotherapy (SCIT), more commonly referred to as allergy shots, and sublingual immunotherapy (SLIT) given as fast-dissolving tablets or as drops under the tongue, which is what we offer here at Nectar.
Allergy drops, which have been utilized since the 1980s, are predominantly used in Europe over SCIT due to safety, convenience, and similar effectiveness. This method of immunotherapy exposes the body to the allergen orally through daily doses taken under the tongue.
Why were allergy drops developed?
The primary reason for proposing and studying alternate routes of AIT administration beyond allergy shots was to improve the safety and convenience of the treatment. In comparison to injections, oral exposure to your allergens is less likely to lead to an adverse inflammatory immune response (i.e. anaphylactic reactions).²
In fact, a recent study showed that of the estimated 1 billion SLIT doses administered worldwide from 2000 - 2011, there had been 11 reported cases of anaphylaxis (all nonfatal).³ In other words, there is approximately 1 case of nonfatal anaphylaxis per 100 million doses administered. This is notably better than the 1 case of anaphylaxis per 1000 injections seen with allergy shots.⁴
In addition to its safety profile, SLIT is easily administered at home. On the other hand, allergy shots are administered via frequent injections, often given 1-2 times per week at an allergist's office.
Are allergy drops an effective alternative to allergy shots?
There is plenty of scientific evidence that shows both treatment modalities successfully treat allergic conditions and manage symptoms long-term when used appropriately. Overall, research has shown that allergy drops are safer, more convenient, and cost-effective. A landmark study evaluating pollen allergies demonstrated that while both modalities have similar effectiveness, SLIT was considerably safer.⁵ Another study evaluated the cost and effectiveness of SLIT vs. SCIT and found that allergy drops were less expensive overall.⁶
What about allergy tablets?
Allergy tablets effectively treat allergic conditions from home but this method is not without its downsides. Allergy tablets treat one allergy at a time, which is highly inconvenient for anyone looking for across-the-board relief. In addition, these tablets are often not covered by insurance or come with a high copay. Since this treatment is relatively more costly, it remains inaccessible to a demographic of patients.
How do I know which allergy treatment option is right for me?
While your doctor may advise one modality over the other, the decision to use drops or shots should be a shared decision between you and your doctor. If you live far from the doctor's office, have a busy schedule, and have a history of severe allergic reactions, or “needle phobia,” SLIT may be a better option for you.
Citations:
¹ Ring, Johannes, and J Gutermuth. “100 years of hyposensitization: history of allergen-specific immunotherapy (ASIT) .” Allergy vol. 66,6 (2011): 713-24. doi:10.1111/j.1398-9995.2010.02541.x
² James, Christine, and David I Bernstein. “Allergen immunotherapy: an updated review of safety.” Current opinion in allergy and clinical immunology vol. 17,1 (2017): 55-59. doi:10.1097/ACI.0000000000000335
³ Calderón, M A et al. “Sublingual allergen immunotherapy: mode of action and its relationship with the safety profile” Allergy vol. 67,3 (2012): 302-11. doi:10.1111/j.1398-9995.2011.02761.x
⁴ Epstein TG, Liss GM, Berendts KM, Bernstein DI. AAAAI/ACAAI Subcutaneous Immunotherapy Surveillance Study (2013–2017): fatalities, infections, delayed reactions, and use of epinephrine autoinjectors. J Allergy Clin Immunol In Pract. 2019;7(6):1996–2003.
⁵ Khinchi, M S et al. “Clinical efficacy of sublingual and subcutaneous birch pollen allergen-specific immunotherapy: a randomized, placebo-controlled, double-blind, double-dummy study.” Allergy vol. 59,1 (2004): 45-53. doi:10.1046/j.1398-9995.2003.00387.x
⁵ Pokladnikova, Jitka et al. “Economic evaluation of sublingual vs subcutaneous allergen immunotherapy.” Annals of allergy, asthma & immunology: official publication of the American College of Allergy, Asthma, & Immunology vol. 100,5 (2008): 482-9. doi:10.1016/S1081-1206(10)60475-9
⁷ Saporta, Diego. “Efficacy of sublingual immunotherapy versus subcutaneous injection immunotherapy in allergic patients.” Journal of environmental and public health vol. 2012 (2012): 492405. doi:10.1155/2012/492405
⁸ Davis, William, MD, et al. “Anaphylaxis in Immunotherapy.” Otolaryngology- Head and Neck Surgery, vol. 107, no. 1, July 1992, pp. 78–83.


